Potential New Testing Methods for Nonalcoholic Fatty Liver Disease
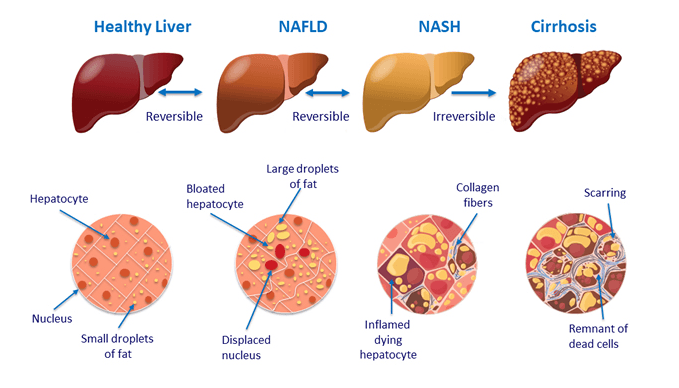
Nonalcoholic fatty liver disease (NAFLD) is a metabolic disease characterized by increased fat deposits accumulating on the liver. People suffering from NAFLD are often asymptomatic until they progress to the later stages of the disease, also known as nonalcoholic steatohepatitis (NASH). NAFLD can also lead to a type of irreversible liver damage called cirrhosis [1]. NAFLD is often physiologically associated with inflammation around the liver, and this leads to a high number of inflammatory proteins known as cytokines [2]. Production of inflammatory control cells known as natural killer T (NKT) cells is also limited [3], and this exacerbates the number of cytokines present because NKT cells are no longer able to control the cytokine population.
Confronting the Hidden Epidemic of Fatty Liver Disease – Holistic Primary Care
While cytokines are known to increase in cases of NAFLD, we must also keep in mind that cytokines are general inflammatory agents. For example, if a subject was negative for NAFLD but recently broke a bone, inflammatory agents will be high in the blood due to the trauma of the bone breakage, which may create a false positive if we are utilizing cytokines to test for NAFLD. This does not mean that testing using cytokines is impossible, but other factors must also be taken into account prior to testing.
Using this knowledge, researchers have developed blood tests to check for early signs of NAFLD. However, the only truly definitive testing method to confirm a diagnosis of NAFLD or NASH is via liver biopsy. Blood tests are able to give researchers a better idea of whether the patient is potentially NAFLD positive, but there is only so much accuracy they can provide. Both of these types of tests can become extremely invasive—particularly biopsies—and therefore, research into urinary cytokine levels as a method of assisting diagnosis of NAFLD is important.
Cytokines were proven to be excreted in the urine in a testable form in 1997 [4]. There was some concern that the filtration system of the urinary tract and the chemical contents of urine, such as ascorbic acid, would degrade the integrity of the cytokines, preventing us from testing for them in the urine. While we are unsure of the relationship between blood cytokine levels and urinary cytokine levels at this time, we are at least certain that cytokines are present and testable in the urine.
There are many different types of cytokines with many different structures. Therefore, it was important to us to determine whether the cytokine interleukin-10 (IL-10) is structurally valid when testing for it in the urine, and to determine whether or not IL-10 levels in the urine trend in a relatively similar pattern to IL-10 patterns in the blood. If our research proved that urinary IL-10 carried the same trends as blood IL-10, this information could be used to provide a more accessible testing method for the general public in regards to NAFLD. In fact, if the hypothesis proved correct, there is even the potential that a urinary dipstick, such as that used in home pregnancy tests, could be designed in order to provide more accessible testing to the general population.
We decided to organize a study to test this theory on 96 volunteers, half of which will be known to be affected by NAFLD. With a blood and urine sample from each volunteer, we will be able to determine the relative potential accuracy of IL-10 as a method of urinary NAFLD testing. If the urine and blood show similar levels of IL-10 between each patient (and patients with NAFLD have significantly elevated IL-10 levels in comparison to the control group), then it could be confirmed that urinary IL-10 is a potential variable that can be used for home testing of NAFLD.
Metabolic diseases such as NAFLD and type II diabetes are becoming increasingly common in Western countries such as the United States. Considering this, increased access to easy and affordable testing is essential. Not only can this increase public awareness of the importance of controlling onset NAFLD, but it can also prevent progressive forms of NAFLD such as NASH or cirrhosis. If the public is able to test for NAFLD at home or in a more affordable way at the doctor, then control of NAFLD will increase as more people are diagnosed and treatment begins.
1) Munteanu, M. A., Nagy, G. A., & Mircea, P. A. (2016). Current Management of NAFLD. Clujul medical (1957), 89(1), 19–23. https://doi.org/10.15386/cjmed-539
2) Haukeland, J. W., Damås, J. K., Konopski, Z., Løberg, E. M., Haaland, T., Goverud, I., Torjesen, P. A., Birkeland, K., Bjøro, K., & Aukrust, P. 2006. Systemic inflammation in nonalcoholic fatty liver disease is characterized by elevated levels of CCL2. Journal of hepatology, 44(6), 1167–1174. https://doi.org/10.1016/j.jhep.2006.02.011
3) Li, Z., Soloski, M. J., & Diehl, A. M. 2005. Dietary factors alter hepatic innate immune system in mice with nonalcoholic fatty liver disease. Hepatology (Baltimore, Md.), 42(4), 880–885. https://doi.org/10.1002/hep.20826
4) SJ, Costello RB, editors (1997). The Validity of Blood and Urinary Cytokine Measurements for Detecting the Presence of Inflammation, 20. Emerging Technologies for Nutrition Research: Potential for Assessing Military Performance Capability. Washington (DC): National Academies Press, Institute of Medicine (US) Committee on Military Nutrition Research; Carlson-Newberry. https://www.ncbi.nlm.nih.gov/books/NBK233764/
- Categories: